
Spot Check
Managing the turbulence of post treatment exams

One spot remained. It’s been the focus of every appointment I’ve had since finishing my cancer treatment in late December. In the four month post treatment PET scan, the spot had ‘lit up’ just as my surgical oncologist, Dr. P, predicted it would. During the follow-up after the scan Dr. P snaked a camera up my nose and proclaimed ‘it looks like a wound, but we can’t be sure.’
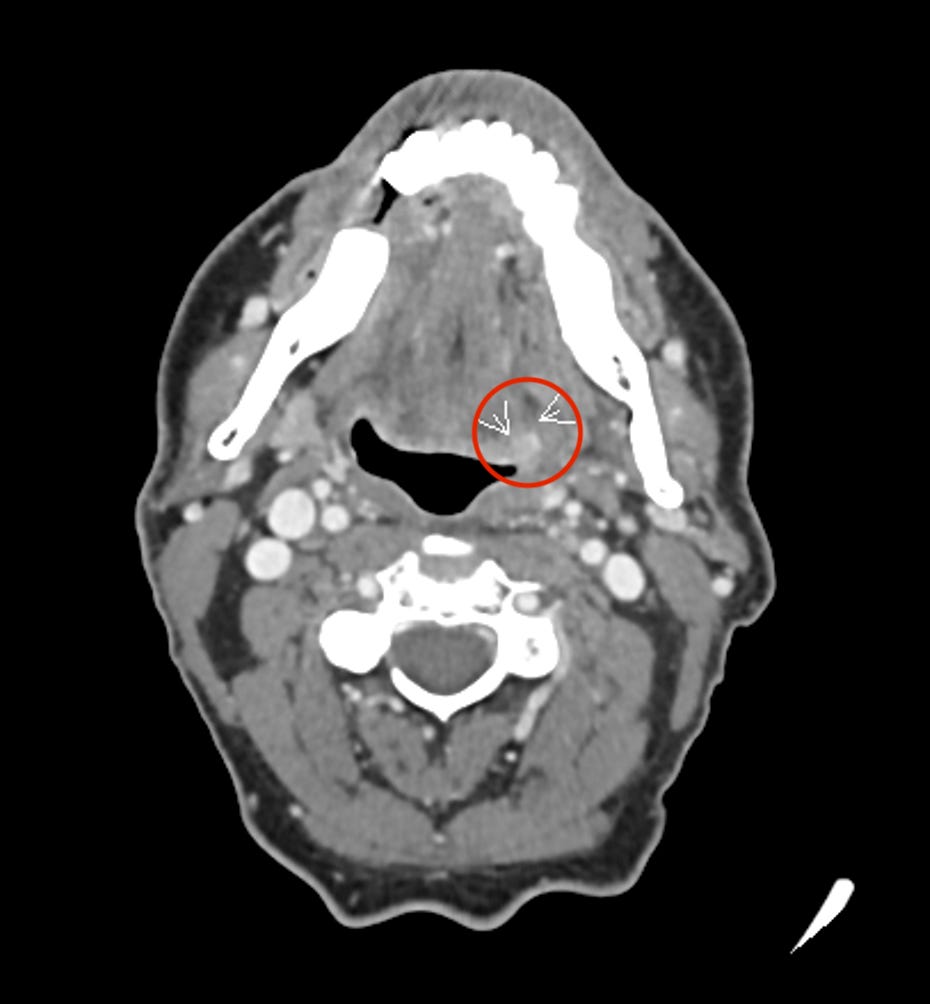
The doctors recommended a CT scan, which showed a 7mm spot of ‘subtle asymmetric enhancement’ that required more investigation. Dr. P took a look at the images while I was on the phone with him going over the results. “Eh, it’s hard to say. It looks like a wound, to be honest,” he said based on the look of the tissue on the scan. “But let’s get a biopsy of it anyways.”
Okay! Better to know right away! The biopsy would be an outpatient office visit just like my first one last July when we discovered the cancer, right? Unfortunately, no. The spot was tiny now compared to the hulky-bulky 4-centimeter beast that filled up my tonsil. I could actually touch my tumor with my fingers. The new spot would be hard to get to. “We need to have you fully asleep.” So full anesthesia. In other words, surgery. Oh boy.
The biopsy was scheduled for next Friday, Dr. P’s surgery day. I knew if the test came back negative for cancer, I’m in remission and I get to move onto the next stage of recovery.
But what if it doesn’t get cleared? “Well, then it gets kind of tricky.” After a long explanation, the main takeaway is you don’t want to do surgery on recently radiated tissue. The spot heals so extraordinarily slow surgeons help it by constructing a flap of tissue from another part of your body. And the area will most likely have much higher levels of bacteria from the radiation, so the possibility of infection goes through the roof. “Expect to be in the hospital for at least five days, maybe longer.” I had a vision of my hospital room, with me climbing the walls trying to get the hell out of there, all while trailing a couple of IV bags behind me. None of this sounded attractive.
After I processed the news, I was calm. The two were such divergent outcomes, but I really believed I had to keep both scenarios alive in my head. As if either outcome could be real. In one life, I go down the road of remission. The other was surgery, recovery, pain, setbacks, and healing, eventually, maybe. Or not.
Friday came quickly. The operation was incredibly short. Jaimee and I walked out of the hospital well before 10 am. I wouldn’t find out results at least for 3-5 business days. When I had my biopsy in July it was two full business days, so if it were the same time frame, we’d get results Tuesday.
Saturday I was fine. Whatever outcome I would live, I told my friends and family. Sunday, less fine, though when Jaimee asked I said I was okay. Monday less fine than Sunday. Jaimee checked in. I said everything was good, even though she could tell it was most definitely not.
I had done the research and dug into the science. I saw that other cancer research facilities, like Memorial Sloan Kettering (MSK) in NYC, were running clinical trials with novel ways of using much less radiation for some patients with my diagnosis, depending on what kind of cells your cancer generated. If your cancer grows incredibly quickly, it can create cells that are starved of oxygen. These cells are very challenging to treat as the radiation requires oxygen to do its job. But for those who don’t have that condition, you most likely need less, and maybe much less, radiation. MSK was treating Oral HPV cancer patients with 60 percent less radiation than what I received. This matters because the radiation (let’s just call it what it is: poison) effects start to get significantly worse the more you receive. Some studies show that the last 5-10 doses of radiation a patient receives is when the terrible side effects start to take root. Like swallowing issues, eating difficulty, saliva gland loss and so many more ugly lifetime impacts. MSK’s internal testing also suggested up to 90 percent of patients had cancer cells that might benefit from less radiation.
With all this, it seemed logical that I probably received more radiation than I needed than less. And that spot in my mouth? That was a radiation wound, which is what all the providers kept mentioning. But try telling that to my brain as it was busy figuring out how to extract myself from the ceiling after being cooped in up a hospital post-surgery to snip out that last bits of cancer. And you don’t really know. Sure, the data looks good, it doesn’t really mean anything. We don’t live in data. We live in how our bodies react to the treatment.
Tuesday was the worst. I had reverted into Cockroach Mode: that oh so endearing (not) method where I put my head down and try to get through difficulties regardless of how I feel. Jaimee noticed and asked directly what was happening. I opened the door a tiny crack a let a little of the pain out. She asked me to open the door wide open and let it out, and I found it hard to do. I did apologize later. When I finally admitted to Jaimee that I was kind of freaking out.
Sure, I was living in both worlds, but I really didn’t want to live in the last mile cancer surgery world. There was the medical stuff to navigate. But even more importantly, what would it mean that the cancer didn’t respond to the huge load of posion my body had swallowed? Does that change the odds of recurrence? Or maybe it never goes away, and I just go into a pain loop with recovery-recurrence-recovery-recurrence cycle. Surgery on radiated flesh is bad. Radiated previously radiated flesh is no fun either.
Everything would be up in the air and there weren’t solid sources of five-year survival statistics based on the other path situation. When it came down to it, I really couldn’t embody this new cancer-odds-world, not fully. There was too much I just didn’t know and honestly didn’t have the emotional capacity to face.
Tuesday afternoon I got a notification on my phone. A new test result was uploaded. I opened up my chart and only saw the words ‘benign squamous mucosa.’ Benign! Then I read the whole thing. No cancer. Just a wound! Tears welled. I felt a warmth creep up my nose. I breathed heavy and put my head in my hands. It had worked! That other world just vanished! I was in remission.
Later when I talked to Dr. P he said there wasn’t much we could do about the wound. It would just need to heal. And of course, it would take time because of the radiation. Since I still had a spot, we would have to keep monitoring it with scans and exams. I had another appointment and CT scan scheduled in two months. It would continue until the wound healed.
And of course there’s the possibility for a recurrence. The data suggests while you can get a recurrence at any time, most of the recurrences happen within two years of the original treatment. If I can just make it two years…. Nevertheless, I’ll have to regularly monitor my health and my mouth. And manage the lifelong effects of the radiation on my body, like jaw mobility and swallowing issues and mouth pain.
But remission. I’ll take it. So we’re all good. Right?
👏👏👏👏👏🫶🏼🫶🏼🫶🏼🫶🏼🫶🏼